A Tale Of Two Omicrons
By Peter Tchir of Academy Securities
I, like many of you, spent part of this long weekend searching for information on COVID and omicron. It is difficult to get good information because:
- Omicron is still relatively new in most areas of the world, and data is limited.
- Very little data distinguishes between Omicron and Delta (as discussed in Chalk & Cheese).
Those are some valid issues that we have to deal with, though I think with some effort, even without more sequencing) we could do a better job of distinguishing between variants.
The big problem I find is that many people don’t want you to know the facts.
- For purposes of today’s T-Report, I will use one set of data. I’ve chosen to use London in GOV.UK. I’ve chosen to use London, because:
- Omicron seems to have been in the U.K. longer than here and the data seems robust.
- London, as a contained area, seems more likely to have up to date data that is consistent across sources. It is in the Northern Hemisphere which is likely useful in extrapolating to the U.S.
- While London has its own quirks (city living, high vaccination rate, etc.), the data and stories that I’m going to tell seem consistent whether we switch to the broader U.K., go back to South Africa, or delve into the data from almost any other country or region (at least that is what I’ve seen so far).
From this data, we will tell two stories:
- The scary version.
- What the data really says.
Cases Are Skyrocketing.
This is true. The number of cases is surging everywhere (actually the number of cases in South Africa has already started to drop, but that isn’t relevant for today’s piece, it is extremely good news, but not a focus for today’s piece).
So, where you want to create fear, or want to dig deeper into the data, there is no doubt that cases are rising. Not only are cases rising, but due to a lack of testing in many places, the cases are being under reported.
Also, and this does cut both ways…
- Cases are even higher because self-testers aren’t reporting.
- Cases are even higher because self-testers aren’t reporting, because they have mild symptoms.
How you choose to describe the under-reporting does make a big difference to the tone of a report. There is no doubt in my mind that cases are heavily underreported right now, but (at least to me,) it makes a huge difference as to why cases are being underreported. In the early days of COVID, there were people very sick who wanted to be tested but couldn’t get tested (that is bad and is scary). Many right now who aren’t able to get tested, want the tests not because they feel bad, but because they need them to travel or to see family (not a scary reason for being underreported). For those who test positive but aren’t particularly sick, the danger as I see it, is that the official data makes all the percentages (hospitalizations, for example) look worse.
Right now, it seems clear that underreporting makes the consequences of having omicron seem worse, and the hype about case counts is largely just that – hype! (we will address the situation of cases and severity amongst healthcare workers shortly).
Hospital Usage Is Rising Rapidly (always expressed as a percentage change)
After cases, which I highly discount, we quickly move into hospital utilization. We are all well aware that swamping the healthcare system is a risk that we want to avoid. So if you want to generate fear, you immediately target this area.
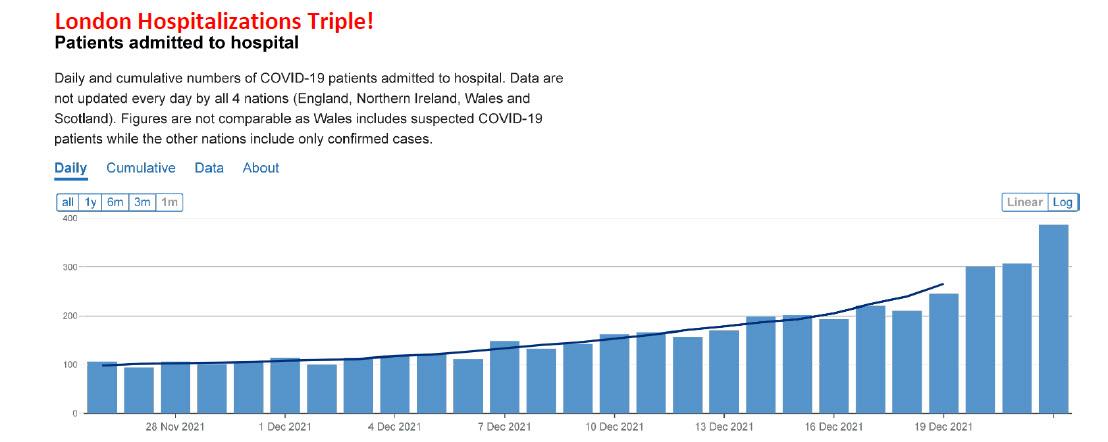
This is factually correct. Since late November, hospitalizations have gone from 100 to 300 (and were still rising on December 24th, the last date for which data was published. The tripling is scary, but it is provided without context.

Daily admittances were consistently above 600 during two prior waves and broached 900 at their peak. While it is possible that Omicron will continue to get worse, the fact is that 300 isn’t as alarming, in the context of where we’ve been, as it sounds. I am not saying that I discount the rise in cases, and I am concerned about their trajectory, but too many pieces stop at the “alarming” tripling and do little to contextualize that in terms of total numbers (300 out of the population of London is manageable).
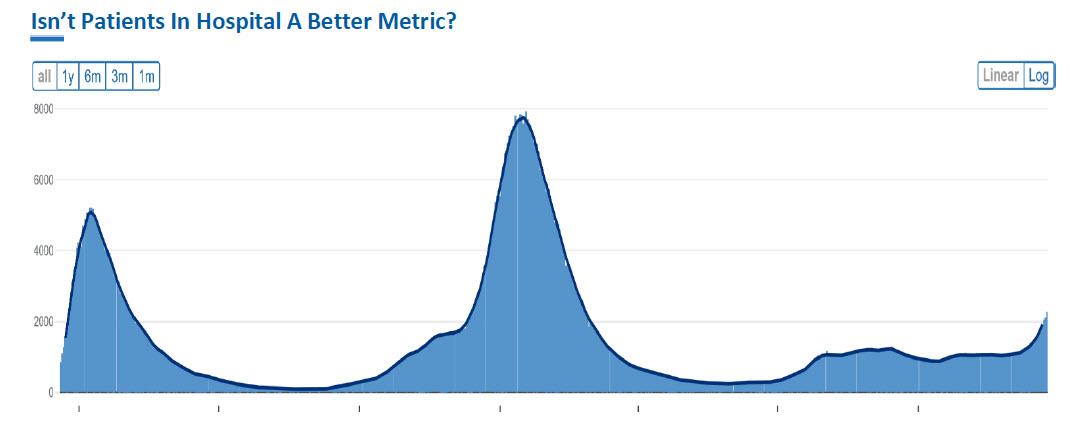
This chart examines the number of patients in hospital. One, it demonstrates that patients in hospital is still small relative to the two prior waves.
What is also interesting, is that there were 1,200 people in hospitals at the end of August and “only” 2,100 now.
Since 200 or so patients have been admitted every day for the past couple of weeks, it seems to me that the much slower increase in hospitalized means that patients are spending less time being hospitalized. There is absolutely zero evidence that people are dying at an incredible pace from Omicron (in fact, very few deaths have been attributed to Omicron), so the only way that the rise in admittances meshes with the reported level of beds occupied is that people are being treated and released relatively quickly.
Where is the length of stay data? So little data is available, even for those inclined to search for it, about how quickly and successfully patients are being treated!
But The Ventilators!
You will find that almost no fear story goes after ventilator usage right now.

Lest I be accused of using longer term data to obscure more ominous short term trends, here is a “better” headline!

This chart seems to indicate that very few patients are needing ventilators.
Part of the reason for this may be that using ventilators has fallen out of favor. That is a possibility as many argued that ventilators seemed ineffective at helping in the recovery process. I’m inclined to believe that improved treatments and lack of severity is why ventilator usage has remained low.
Gotcha #1 – Lag Effects
Yes, there is a lag from the time that someone becomes infected, to the time that they test positive, to the time that they need hospitalization, to the time that they need ventilation. Those are all legitimate concerns. The fear story argues we just haven’t had time to experience the severity.
That is a risk, but it is why I chose London rather than the U.S., because we should have seen some of those issues come to fruition for the fear side of the equation.
Also, now is a good time to bring up South Africa, which has been dealing with Omicron longer than almost any other country.
According to the WHO, cases in South Africa are already potentially tumbling (though we need to see if the holidays impacted those results), but more importantly, death from COVID never spiked during the Omicron wave. For the first time, at least in South Africa, the chart of cases versus the chart of deaths has no correlation whatsoever. While the “lag effect” might have some merit in London, it has been quashed in South Africa, and for a period of time every positive story about South Africa was accompanied by admonishments to not get comfortable because of the lag.
The lag effect was a more legitimate concern two weeks ago than it is today, where it really does seem to lean heavily towards fear mongering rather than anything the data is telling us.
Gotcha #2 – Long Covid
Even the stories that begrudgingly admit that the current data isn’t so bad, seem to end with stoking our fears about long term covid. Yes, some people with previous variants have suffered from long covid. That is awful, but the two things that I keep thinking about are:
- Does this variant pose the same threat of long covid? If it has mutated to something far less severe, is it possible that it is less likely to leave victims with long covid? I am not sure about the answer to that, but since the fears about this variant seem to have been wrong (so far), I think we need to wait and see before panicking about long covid.
- I have no reason to believe that we won’t find treatments for long covid over time. The medical community has been attacking covid on many fronts. While we all know about the vaccinations and boosters (more on that later), we are seeing more and more treatments being developed. From single pills to effective treatments using a multitude of pharmaceuticals, we have many more tools to help those infected. As the world’s attention shifts to long covid, there is no reason to expect failure. I am strongly in the camp that long covid, while an issue today, is something that will be addressed in the coming months and quarters. Yes, that sucks for those who have it today, but assuming long covid is permanent seems overly pessimistic and betting way too heavily against modern science.
What About Healthcare Workers?
This is a legitimate concern. If healthcare workers are hit hard by Omicron, we could see a rapid decline in availability of hospital beds and treatments. It is something that the fear side has correct, to a large extent.
But the CDC updated guidelines on December 23rd start to address this. They already are easing some restrictions on healthcare workers and they caveat the updated guidelines with the statement that “isolation time can be cut further if there are staffing shortages).
Personally, I suspect that if the CDC was scared of this variant’s severity, they wouldn’t be so quick to change the rules. They have to balance the availability of care, with the safety of healthcare providers. Maybe I am reading too much between the lines here, but I suspect that the CDC understands that the severity is lower and that is influencing their policy regarding healthcare workers.
It is “Prudent” For Governments to Stoke Fear
Ahead of the holiday season, when gathering and traffic are at their peak, governments across the globe have no interest in encouraging a potential spike. They know how easily Omicron is transmitted, and so long as they have any doubt about the severity or the ability of the system to handle the already likely surge, they have no interest in encouraging more spread.
As mentioned in “Last Thing I Wanted to Write About is Omicron”, public policy already pushes their modelers to “worst” case scenarios. So even if governments thought Omicron is less severe, they will not encourage that viewpoint, at least not until after the holidays.
So, I would expect every government proclamation to err to the cautious side, and even with that bias (which is a rational bias), we are seeing positive headlines come out.
I expect that once we get through the holiday crush, we will see a change of tone from officials as their fear of a holiday induced spike recedes and we can all dig deeper into the details. Remember, President Biden’s address on Tuesday seemed to be skewed towards the realization that people need really good reasons to enter another lockdown.
Vaccines, Boosters and the Unvaccinated
I don’t even want to enter into this can of worms. This is one area where we would benefit so much from the details begged for in Chalk & Cheese, but the reality is that we don’t have that level of granularity.
- Vaccines and boosters seem to help reduce the severity of all types of COVID including Omicron.
- For many, the wave of infections in vaccinated people and the ability of vaccinated people to spread Omicron seems to be above levels that public perception thought was likely. This is to a large degree an issue over the messaging surrounding what the vaccines can and cannot do that needs to be better addressed, especially as we seem to be moving to a 4th booster for many, and quarterly boosters not out of the realm of possibility.
- Omicron at least, doesn’t seem that bad for unvaccinated people. While there is “worry” that this only encourages fewer vaccinations for me, at the moment, it seems like a huge victory for us as it is one reason that Omicron (with its high transmissibility), isn’t causing severe illness and death to escalate.
The battlelines around vaccinations have been firmly established, and I suspect that little about Omicron will changes those battlelines significantly given the bullet points above.
Since this is such a touchy subject (that I am attempting to dance around), I feel that it is appropriate to disclose that I have had two shots but am a couple months behind on my booster (and the rest of my family has original vaccinations and is up to speed on recommended boosters).
The Next Variant Could Be Worse.
So far, it seems like Omicron is mild compared to earlier variants. While there is a strong tendency for viruses to mutate to less dangerous versions, there is no guarantee of that. While viruses are mindless, their mutations are effectively “solving” for how to propagate their species. Killing a host too quickly isn’t a particularly successful strategy for propagation. Ebola, for example, is so deadly and transmissible, that it could wipe out mankind, except its sheer virulence tends to be self-defeating in its efforts to propagate (it kills entire populations so quickly that it doesn’t spread as much as it could, relative to how transmissible it is). Assuming for the moment, that Omicron isn’t that severe, we have to take this victory (and it is a victory) and use the time to ensure that any shortcomings that were obvious in how we have dealt with Omicron be fixed for future variants. And while I’m not necessarily a fan of ‘worst case’ scenario modelling for public policy, I do think that being properly prepared for worst case scenarios is a good public policy goal.
Bottom Line
Hopefully, the Tale of Two Omicrons, provides a helpful framework for digesting news and headlines in this environment. Markets were already ahead of politicians and the mass media in estimating the severity of Omicron, so there is a limited rally left in that.
While this shortened week is more likely to continue with last week’s strength (seasonality, more good news on Omicron getting published than bad news, etc.), we then have to turn to the economy, consumers, less helpful central bank policy and what is or isn’t truly priced in.
In the meantime, enjoy this holiday season and be happy and grateful that Omicron does seem mild.
Tyler Durden
Mon, 12/27/2021 – 13:12
via ZeroHedge News https://ift.tt/32Edxam Tyler Durden