Saturday Night Fight… At The Pharmacy
Via Pierre Kory’s Medical Musings Substack,
In the Omicron wildfire, with hundreds of thousands ill each day, U.S physicians and patients need their pharmacists support.. but most block access to generic medicines, fearfully and/or willfully.

I am exhausted.. physically and emotionally and morally. Although I am not sure moral exhaustion is “a thing,” the daily witnessing of masses of physicians and pharmacists abandoning their core responsibility of placing the welfare of the patient as their primary consideration.. is beyond wearying. As my friend and COVID expert Dr. Hector Carvallo has long ago said, “it’s time for the lawyers.” It is becoming increasingly critical that the law profession aid the medical profession as it has long ago been led astray by captured federal pharmaceutical agencies. Note that I no longer call them “federal health agencies” as all their actions have been 100% consistent with what a pharmaceutical or vaccine manufacturer would want them to do. To prove that point, I simply ask that, when you read an announcement in corporate media that reports a new decision or action by the federal pharmaceutical agencies (FPA’s for short), simply ask yourself “is that what a pharmaceutical company would do?”
Perfect example of this exercise was 2 days ago when it was announced that the “FPA” had authorized boosters for 12-17 year old’s against omicron (a generally mild cold in kids), using a vaccine designed for older, fundamentally different variants that have already spectacularly failed at giving protection against omicron given ever-increasing data of “negative efficacy” (i.e. vaccinated people are getting omicron more frequently than the unvaccinated). Yet the FPA “doubles down” with yet another “non-scientific policy” so that Pharma can increase the total market size of those eligible for a vaccine… and who cares if this decision ends up sending more kids to hospital than the disease ever would. Another brutal assault on public health. Another day in the United States of Pharma.
In the United States of Pharma, individual docs and pharmacists have been led so far astray, forgivably or unforgivably, due to the relentless barrage of dis-information targeted at them by the FPA’s (further supported by relentless, daily propaganda appearing in both major media and medical journals). The resulting proportion of these two professions that have failed to display even a modicum of either critical thinking or moral conviction.. is terrifying. It is also causing lots of problems for patients and physicians (a colleague of mine now differentiates “doctors” from “physicians”, reserving the latter term for those who follow our guiding principles and ethics by always, always, putting the patient’s welfare as their primary goal above all else, even at personal sacrifice).
What prompted me to write this substack was my most recent failure (and the resulting distress that led to crap sleep last night) over not being able to get a pharmacist to fill my orders in the hours prior to closing of pharmacies for an acutely ill COVID patient that had contacted me reporting high fevers, sore throat, and body aches. I immediately wanted to start him on a short course combination regimen of three, old, safe, cheap generic medications, all with large clinical trials evidence bases showing high efficacy against COVID (ivermectin, hydroxychloroquine, fluvoxamine). What is important to note is that, months ago I stopped trying to contact ANY pharmacy unless I KNEW they would fill my scripts for these off-patients medications because unless I knew a pharmacy was “safe”, I ran a high probability of entering an un-affordably time-wasting and ultimately losing argument with some smug, obstinate pharmacist. As a result, we early treatment docs have long since been forced to build lists of “safe haven” pharmacies where we know we can easily get access to these medicines for our patients.
However, last night, I was inspired to make an attempt on a new, unknown pharmacy on behalf of my new patient as I had just read Steve Kirsch’s substack about my colleague and early COVID-treatment pioneer/expert Dr. Brian Tyson, in which was included the letter written by Dr. Brian Tyson’s attorney (also with the last name Tyson) that was used to “sway” a local pharmacy that had suddenly refused to fill.
The letter is thorough , deeply well-argued, and informs the pharmacists that they are; 1) violating the civil rights of patients, 2) interfering with a physicians ability to practice medicine and 3) exhibiting behavior that constitutes the unlicensed and negligent practice of medicine. Now, I had argued all these points before in previous “conflicts” with pharmacists, but never all at the same time, and rarely threatening a lawsuit. Duly and newly emboldened.. I made the call.
4:20 Pacific time (pharmacies close there at 6pm).
Transcript (from memory):
“Hi, I’d like to call in a prescription for a couple of patients.”
“OK, what’s the first patients name and date of birth?”
“Timothy Thomas (not his real name), born Nov. 6th, 1977.”
(pause, clacking of keyboard)
“OK, what does he need?”
(Wait for it)
“He needs ivermectin, 3 milligram tablets, I want him to take 15 each day as he is a big guy, and for 5 days with a refill. Then he needs, hydroxychloro…
“Doctor, I am sorry but I cannot fill the ivermectin. The owner has said we are not to fill for COVID, there is no evidence it works.”
“Listen, I don’t know who the owner is but you are the pharmacist on duty, and I am calling in a prescription to you, not the owner.”
“I,I, I am sorry but I can’t..”
I look at the letter, and then start spewing rapid fire arguments at him, “well unfortunately for you, my patient is an executive of a company and their lawyer is prepared to and will send a letter of intent to sue if it has not been filled because you are violating his civil rights, blocking my licensed ability to practice medicine and care for my sick patient, and you are clearly practicing medicine illegally and highly ignorantly. You should at least know what you are doing if you are going to do it without a license man”
“But I am allowed to refuse doctor.”
“That is what you think and what you have been told… But, I can promise you, that when you bring your arguments up in court as to why you refused, they will not hold up if any harm comes to my patient by your refusal. They will NOT HOLD UP, but you can try. The lawyer will serve the letter on Monday, I promise you, we are fed up out here and are fighting back, all of my fellow physicians being blocked by pharmacists are now using legal action (OK, so I overstated things a bit), I am sorry you are in the position you are in, but you have no rational or scientific evidence to support a refusal, but if you want to go to court to find out, we can make that happen for you”
“I..I.. feel intimidated.”
“Well, I am sorry for that, but you are hurting my patient and my ability to care for them. It is THEY who YOU are intimidating Sir. All you have to do is take my script, fill it, and we don’t have to go on like this. These medications are FDA approved, I am using them off-label based on a large body of evidence and experience in COVID, and off label prescribing is both legal and historically encouraged by the FDA. You are clearly practicing medicine and I promise that will be proven to you in a court of law. Please just fill it and you wont have to hear from me or my patient again.”
(Pause, silence)
“I cannot do it, I am not supposed to.”
“OK then, I will also remind you that you are legally required to provide me your name and license number as we will be pursuing legal action against you.”
“I am not giving you my name, I am not comfortable with that.”
“OK, so you think I can’t find it out? Fine, I am also documenting this refusal. Again, I am not interested in a contentious argument, I am asking you simply to fill the prescriptions for two sick patients who need my help, and if you do, you won’t have to hear from me or the patient’s lawyer.”
He whispers.. “OK, tell me the rest of the prescriptions.”
I tell him the rest, then say, “my patient will be there by closing time, thank you and I apologize for my tone but I am just trying to do the best for my sick patients.”
Victory? Yes! Haven’t won one of these in months.. the letter and it’s well articulated legal threats worked! Thanks Steve! Thanks Bryan (and your attorney)!
I finish telling him the rest of the scripts for my patient and his wife (I also needed to call in medicines for her so she could have some on hand and also begin ivermectin as a prophylactic agent given it ensures an easier course even if she is already or eventually becomes infected).
I then happily call the patient, tell him to get his wife to pick up the medicines along with the other over-the-counter compounds that have clinical trials supporting their use. And then I go to the couch to literally lay down (insane day of dozens of patient care requests, other zooms and phone calls, maybe 12+ hours on the phone).
30 minutes later.. patients texts me.. my wife went there and the pharmacist wont fill.
Now, despite the fact that I co-wrote a document with Executive Director Kelly Bumann of the FLCCC and Unity Project Founder Jeff Hanson, called “Overcoming the Barriers to Access,” which is a document full of sound, pragmatic tactics and dialogue examples offered to patients (and docs) in order to help them navigate such pharmacist obstructions, they typically will not work when it is an hour before closing on a weekend. So, here I am the next morning. Fortunately I was able to get 2 of the medicines filled through another pharmacy, with enough for his wife as she unsurprisingly fell ill overnight (omicron moves fast). Unfortunately, they will have to wait until tomorrow to get the 3rd medicine from a “friendly” or “underground” pharmacy (not really underground but you get the analogy).
This is what it is like out here trying to fight for patients sick with COVID – widespread delays in care as blocking access to medicines by ignorant/arrogant pharmacists is ubiquitous. The majority of pharmacists (not all!) have simply stopped thinking critically or devoting effort to review the evidence base, instead simply believe what they are told by their Boards (a.k.a. their Ministries of Truth). As if the insane numbers of ill omicron patients to care for is not challenging enough.
In the words of Louisiana Attorney General Jeff Landry, who went after his state’s Pharmacy Board when they tried to scare the states pharmacists away from prescribing ivermectin by sending them threatening letters, “it is shocking that pharmacists are suddenly developing a conscience after spending the last decade handing out opiates like they were M & M’s”. Well said and tragically absurd.
This newfound conscience influencing such actions is likely further fueled by a sometime resident psychology of pharmacists who may feel “less than” a physician given their limited scope of patient care tasks. Emboldened by a seemingly legal opportunity to assert superiority and control over physicians, many find these too irresistible to resist. Instead, they seem to be clearly “getting off” from pointing out to the “stupid” doctors that the Ministry of Truth has done the research for them and have found that in the name of science, doctors must be stopped from using “ineffective horse de-wormer” to treat COVID. Good times. Just another day in the life of an early COVID treatment expert.
Let me end with the following disturbing data and observations. Take a look at this chart compiled by the FLCCC data analyst, Juan Chamie.
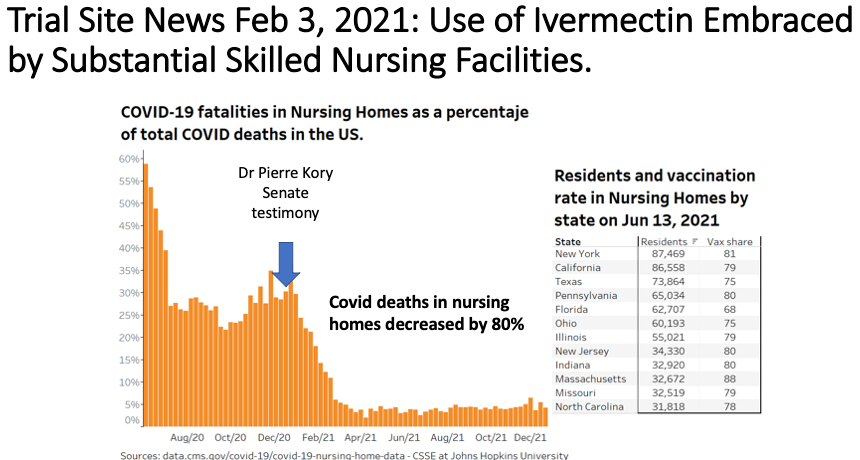
From the above, it should be noted that prior to our FLCCC ivermectin paper being posted on a pre-print server (Nov 13, 2020) and prior to my testimony in the Senate hearings of Senator Ron Johnson noted above (Dec. 8, 2020), nursing home residents made up about 30% of all COVID deaths in the U.S. (also note that Senator Johnson’s efforts have made him one of the most (if not the most) impactful of the early treatment advocates for COVID in this country.. (and in history?).
As you can see from above, suddenly, by mid-to-late December 2020, the proportion of dying U.S COVID patients that were residents in nursing homes started to plummet to now around 5-6% of all U.S COVID deaths.. and it has stayed stably low at this level ever since (notice how you never read any more newspaper reports of legions of people dying in nursing homes?). Hmmm. Was it the vaccines? Nope – nursing home resident vaccination rates were equal to or lower than the over 65 non-nursing home population, and the latter continued to make up a large proportion of COVID deaths in the U.S. So, why did nursing homes become such “safe havens” relative to the rest of society after December of 2020?
I maintain there are two reasons; 1) nursing homes often have their own in-house pharmacy so do have to rely on negotiating with arrogant/ignorant retail pharmacists for access to medications like ivermectin, and 2) nursing home directors across the country learned that ivermectin is highly effective at preventing hospitalization and death, and thus they have widely used it across the U.S to treat COVID outbreaks in nursing homes (here, here, here, and here). Turns out, this practice makes for really good business since dead or hospitalized nursing home residents.. no longer generate income for the nursing home. Once again, all about the Benjamins. Shocker.
* * *
Tyler Durden
Mon, 01/10/2022 – 21:10
via ZeroHedge News https://ift.tt/330pDeP Tyler Durden