Food Bank Strains Emerge As Economy Falls Off Fiscal Cliff Tyler Durden
Tue, 08/11/2020 – 22:25
The latest economic data suggest the US recovery stalled. One look at the Citi US econ surprise index, as of this week, shows the recovery ran out of steam last month. A fiscal cliff is already underway, set to enter the second week on Friday (Aug. 14) as tens of millions of Americans are unemployed and have yet to receive their stimulus checks.
The recovery, so far, is a massive economic sugar rush, entirely a function of the Trump administration on a reckless spending spree. One way the administration can artificially supercharge consumption is through issuing direct transfer payments to the working poor. The extra money has been used by households to pay down credit card bills, put food on the table, and pay housing expenses, while others used the free money to buy automobiles and FANG stocks.
President Trump signed an executive order over the weekend to fund another round of stimulus checks of approximately $400 per week, a reduction from the $600 federal aid seen in the first round from March to the end of July.
Massive federal spending has transformed America into a welfare state under the GOP watch. Tea Party politicians aren’t pleased with the Republican establishment’s wild spending spree.
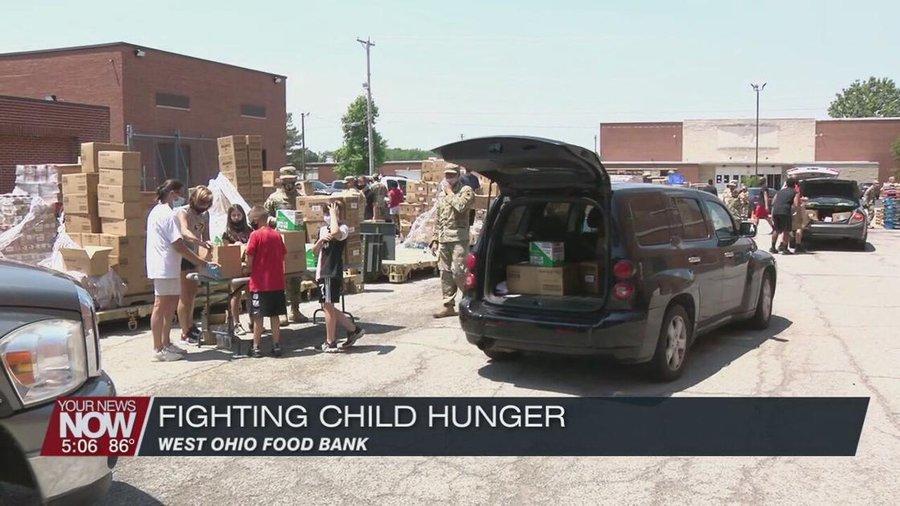
With a fiscal cliff coming up on the second week, tens of millions of folks are unable to consume because they are insolvent and jobless, and their amount of consumption is dependent on the government. We’ve noted before, a quarter of all household income is derived from the government. And with no stimulus checks in the mail, that means Americans are returning to food banks:
Claudia Raymer, who manages a network of food-security groups in Ohio County, West Virginia, told Bloomberg when stimulus checks stopped arriving in late July, there was an immediate impact on households, resulting in rising food bank activity among the working poor.
The fiscal cliff will be more damaging in lower-income communities (than major metros), such as small towns in West Virginia, where folks were being paid handsomely by the federal government to sit at home. The problem is, once the payments end, consumption plunges, and the local communities return to a recessionary environment. With federal aid already running out for the stimulus program, the fiscal cliff has already been realized in West Virginia:
“We’ve definitely already seen food-security needs increase, just in a week, since the extra unemployment has ended,” Raymer said.
Treasury Secretary Steven Mnuchin said Monday the next round of stimulus checks could take a couple of weeks to distribute, which would suggest households might not receive their stimulus checks until the end of August.
Days before the stimulus program ended (late July), a sizeable food bank line appeared in Baltimore, Maryland.
behind the scenes: food bank line in Baltimore just getting started – a lot of hungry and broke families as fiscal cliff begins pic.twitter.com/30C1OBJDSP
— Alastair Williamson (@StockBoardAsset) July 26, 2020
The economic crisis is far from over. Households are entirely screwed as depressionary unemployment levels will continue into the election. Many folks are dependent on direct transfer payments from the government and food banks for survival. Who would’ve ever thought this would be the case in the “greatest economy ever.”
via ZeroHedge News https://ift.tt/33TDhOG Tyler Durden
Shell-shocked is a good way to describe the mood in the U.S. for a good part of the Spring of 2020. Most of us never thought it could happen here. I certainly did not, even though I’ve been writing about pandemic lockdown plans for 15 years. I knew the plans were on the shelf, which is egregious, but I always thought something would stop it from happening. The courts. Public opinion. Bill of Rights. Tradition. The core rowdiness of American culture. Political squeamishness. The availability of information.
Something would prevent it. So I believed. So most of us believed.
Still it happened, all in a matter of days, March 12-16, 2020, and boom; it was over! We were locked down. Schools shut. Bars and restaurants closed. No international visitors. Theaters shuttered. Conferences forcibly ended. Sports stopped. We were told to stay home and watch movies…for two weeks to flatten the curve. Then two weeks stretched to five months. How lucky for those who lived in the states that resisted the pressure and stayed open, but even for them, they couldn’t visit relatives in other states due to quarantine restrictions and so on.
Lockdowns ended American life as we knew it just five months ago, for a virus that 99.4-6% of those who contract it shake off, for which the median age of death is 78-80 with comorbidities, for which there is not a single verified case of reinfection on the planet, for which international successes in managing this relied on herd immunity and openness.
Still the politicians who had become dictators couldn’t admit such astonishing failure so they kept the restrictions in place as a way of covering up what they had done.
That shock of Spring has now turned to a Summer of wickedness, with everyone pointing fingers at everyone else for the sorry state of life. Patience has run out and a national viciousness has taken its place. It is evident not only online but in person where strangers scream at each other for behaving in ways in which they disapprove.
What many states are calling “open” today would have been called “closed” six months ago. Sports are rare. Theaters aren’t open. In some places, you still can’t go to gyms or eat inside. Mask mandates are everywhere, and mask enforcers too. People are ratting out their neighbors, sending drones to ferret out house parties, and lashing out at each other in public places.
In a mere five months, lockdowners have manufactured a new form of social structure in which everyone is expected to treat everyone else as a deadly contagion. Even more preposterously, people have come to believe that if you come closer than six feet of another person, a disease spontaneously appears and spreads.
America has become an extremely ugly place. This is what lockdowns did.
All of this has occurred in the midst of the greatest political divide in many generations. Oddly, you almost predict a person’s politics based on their attitude toward the virus, as if sitting political figures are responsible for creating or controlling pathogens that have been part of the human experience since we first walked and talked. The politicization of this disease has been a terrible noise that has distracted from the wise disease management that characterized the American way for more than a century.
But the American people support this, right? I’m not so sure. It’s true that the TV and online media are blaring panic all day every day. If that’s where you get your information, it surely must feel like a plague. There is also the problem that people feel tremendously powerless right now. They have been locked down, silenced, humiliated, brutalized. The few attempts to get out and protest the lockdowns were greeted with jeers and derision by mainstream media. But it turned out that this was because they were protesting the wrong thing. When the protests against police brutality and racism swept the country, the media wholly approved. Yes, it all felt like gaslighting.
Where precisely does American opinion stand on lockdowns today? The polls one cannot trust: people know exactly what they are supposed to say to pollsters during a police-state lockdown. It’s usually a good guess that one-third of Americans take a position that is more-or-less consistent with human liberty – it’s not a fixed group and it shifts depending on the issue – so that’s probably a good guess now.
The incredible frenzy of the lying media has confused vast numbers. A poll revealed that many Americans think that 9% of us have died from C-19 whereas it is really 0.04%.
So yes, we have a propaganda problem, starting with the New York Times, which just today…
…demanded “more aggressive shutdowns than have been carried out in the past. The United States has not had a true national lockdown, shuttering only about half the country, compared with 90 percent in other countries with more successful outbreak control.”
None of which is true. This is pure ideological propaganda. The people who are saying true things seem to be only the 1% vs. the barrage of nonsense coming from media culture today.
We see almost no discussion in the mainstream press of the empirical evidence at home and abroad that the lockdowns make no sense from a medical and economic perspective. Medical experts for many decades have warned against disturbing social functioning in the event of disease. Preserving freedom has always been the policy priority: 1949-52, 1957-58, 1968-69, and 2005. The American revolution itself took place in the midst of a smallpox outbreak. Liberalism arose during centuries of pandemics.
And yet here we are.
This country needs a serious anti-lockdown movement, one that is not just political but cultural and intellectual, one that is deeply educated on history, philosophy, law, economics, and all sciences, and can rally around traditional American civic postulates concerning individual freedom and the limits of governments, and also around universal principles of human rights. If liberty means anything, it means that we are not locked down. It means, moreover, that lockdowns are unconscionable.
What should this movement – which need not be formally organized – study, believe, and teach?
Because property rights are the first violated in lockdown, the movement needs to embrace and champion the right of private ownership and control: of businesses, homes, and ourselves. The liberal tradition has long affirmed this principle, and it is nothing but appalling that the lockdowns took place as if private property doesn’t exist. Suddenly everything and everyone belonged to the state, and it would be the state to declare what is or is not essential, or even what is elective vs. nonelective for your medical care.
It should embrace the freedom to choose our associations, since that is what came under attack next: we couldn’t gather in groups, hold conferences, go to the movies, do anything not “socially distant” (I’m so sick of that phrase, wth dubious origins, that I could barely type it), or even go to another state to visit friends and relatives.
This movement needs to celebrate and defend religious freedom, since, incredibly, most houses of worship were forcibly closed by government. The modern idea of freedom came about in the late Middle Ages when exhaustion from religious wars gradually gave rise to the idea of tolerance. Religious toleration was the first great freedom that came to be codified in law. It’s stunning that it was so flagrantly violated this year.
It must come to terms with free enterprise and the innovation that comes with it. How much wealth and creativity has been lost in the lockdowns? It’s unfathomable. The biggest victims have been small and medium-sized businesses, whereas the large tech firms have thrived. To start and manage a commercial enterprise is a human right, the realization of which was the great achievement of modern life, as it spread prosperity throughout the world and lifted up the world’s people from the state of nature and to levels of the entrenched hierarchies of old.
Part of this liberal ideal is free trade, which has come under fire from both the left and right. Don’t forget that Donald Trump kicked off this dictatorial frenzy with his sudden and shocking bans of travel from China and Europe, which resulted in a frenzied and frantic mass crowding of airports in the days following. He did it with a stroke of a pen, overriding all his advisors. He still brags about it.
How much did his extreme reaction here inspire governors to do the same? Of course his actions reflect his persistent isolationism on not only trade but immigration too. Even now, Trump is refusing to allow foreign workers into the U.S. (except for emergency cases) because he incorrectly believes this will help the American job market. It’s an outrage: free enterprise entitles the employment of anyone from anywhere. This is a policy that is good for everyone.
So long as we are talking about freedom fundamentals, let’s talk about masks. They have become exactly what the New England Journal of Medicinecalled them: a talisman. They are symbols of social commitment and political loyalty. A free society rallies around individual choice, so if masks make a person feel safe, or if it makes them feel they are keeping others safe from their breath, fine. But when people attack others for resisting wearing them, and are apparently upset at the seeming appearance of rebellion from rules, this is imposition and intolerance – perhaps understandable given the times, but still illiberal.
Laws requiring face coverings in public would never have been tolerated even six months ago. And yet here we are, not only with laws but a growing number of recruits within the public to enforce them with appalling rudeness. It’s hardly the first time in history. American sumptuary laws in Colonial times mandated that people not dress in fancy clothes for reasons of piety and social conformism. Part of the capitalist revolution included the freedom to dress as one wants and the mass availability of fashion for everyone. The mandatory mask movement and its shock troops among the public is but a revival of puritanism.
The lockdowns crushed the economic prospects of millions, and government attempted to make up for that with wild spending of other people’s money and an unprecedented use of the printing press, as if government can somehow paper over the destruction it caused. Therefore, the anti-lockdown movement needs a commitment to fiscal sanity and sound money. We now know that a government with the capacity to create unlimited amounts of paper money cannot be constrained. This needs to be fixed.
As for health, the topic or excuse that unleashed the lockdowns in the first place, we surely should learn from this experience that politics and medicine need to be separated with a high wall. We have medical professionals who are traditionally in charge of mitigating disease, and they do so in line with their own professional associations and best judgement. Politics should never override the doctor/patient relationship, nor presume to know what is better for us than our own physicians.
On the matter of education, governors all over the country cruelly locked down all the schools, though there is near-zero threat to kids from the virus and there is no verified case of a child passing C-19 to an adult. Perhaps a small silver lining is that we have learned more about how parents can exercise more control over education than they have previously had. The anti-lockdown movement needs to embrace a multiplicity of educational alternatives including the possibility of full privatization so that education can again be part of the free enterprise matrix.
It’s true that anti-lockdown carries a negative connotation. Is there a better word to convey the positive dimension? My preference: liberalism. Progressives have abandoned it. It is also correct from a historical and international perspective. Liberalism and modernity are inextricably linked in history, says Benjamin Constant. A liberalism of the future needs to be prepared to understand, advocate, and fight for freedom in a non-lockdown world. No exceptions.
Which takes us to the final point. Whether this movement is working in the realms of academia, culture, journalism, or politics, there is an absolute urgency that it exercise unrelenting moral courage and integrity. Ferociously. It should be uncompromising on crucial points. It must be willing to speak even when it is unfashionable to do so, even when the media is screaming the opposite, even when the Twitter mob floods your notifications, even when you are shamed for thinking for yourself.
This time around, as you have surely noticed, even the voices of good people with good ideas fell silent in fear. This fear must be banished. The blowback against this despotism will come but it is not enough. We need character, integrity, courage, and truth, and this perhaps matters more than ideology and knowledge. Knowledge without the willingness and courage to speak is useless, because (as E.C. Harwood taught us) for integrity there is no substitute.
In the end, the case for unlocking society is a spiritual matter. What is your life worth and how do you want to live it? How important are the hard-won freedoms you exercise daily? What of the lives and liberties of others? These are everything. Freedom has never prevailed without passionate and courageous voices to defend it. We have the tools now, many more than before. They can throttle us but can’t finally shut us down. The notion that we would fail to speak for fear of the Twitter mob is absurd.
This movement, whether it is called anti-lockdown or just plain liberalism, must reject the wickedness and compulsion of this current moment in American life. It needs to counter the brutalism of lockdowns. It needs to speak and act with humane understanding and high regard for social functioning under freedom, and the hope for the future that comes with it.
The enemies of freedom and human rights have revealed themselves for the world to see. Let there be justice. The well-being of us all is at stake.
via ZeroHedge News https://ift.tt/30OY8AE Tyler Durden
University Of Georgia Suggests “Wearing A Face Mask” During Sex Tyler Durden
Tue, 08/11/2020 – 21:45
Just when you thought all universities were good for was churning out uninformed Marxists, the University of Georgia breaks that stigma by offering up some groundbreaking sexual health advice in the midst of the coronavirus pandemic.
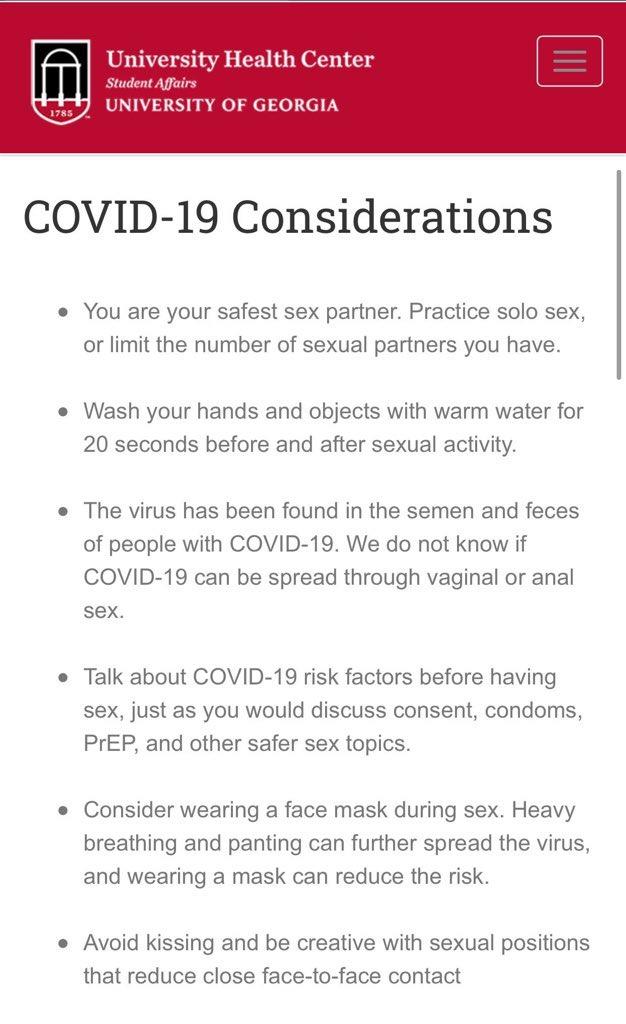
The University had written a section called “Covid-19 Considerations” on its University Health Center website several days ago, but the document was pulled down after the university was subjected to ridicule for its content, which actually suggested “wearing a face mask during sex.”
“Heavy breathing and panting can further the spread of the virus and wearing a mask can reduce the risk,” the entry on the site had said.
The site had also suggested practicing “solo sex”, which we’re guessing is now the gender-neutral politically-correct-approved non-binary non-triggering term for what used to be called masturbating. “You are your safest sex partner,” the site said.
The site offered up other confidence inspiring notes like “Wash your hands for 20 seconds before and after sexual activity” and “We do not know if Covid-19 can be spread through vaginal or anal sex.”
Happy to see that tuition money going to good use…
Meanwhile, peers at the University of Maryland have disagreed and said that wearing a mask is “not likely to prevent transmission if one of the partners has COVID-19” on their website.
“The information was consistent with language that appears on multiple health and medical sites across the country, including the Mayo Clinic. However, when the information was mocked, ridiculed and criticized on social media, we decided to take it down.”
via ZeroHedge News https://ift.tt/3fJu11W Tyler Durden
“Never let a crisis go to waste,” the old adage goes, and the coronavirus fiasco has demonstrated this principle in action more times than one can count. From declarations of veritable society-wide house arrest to crazed government spending and monetary policy, there has been no shortage of opportunistic actors working to live out their dreams of power and dominion over others that “normal” times would not allow.
Another such instance of gleeful advantage taking has come to light in the form of the Pennsylvania Department of Health’s “Ethical Allocation Framework for Emerging Treatments of COVID-19” guideline, a document that barely conceals its authors’ desire to use the current fiasco as an opportunity to engage in their own schemes of egalitarian social engineering.
Just as a reminder of the kind of central planners we are dealing with, this is the same Pennsylvania Department of Health that decreed on May 12 that nursing homes “must continue to take new admissions, if appropriate beds are available, and a suspected or confirmed positive for COVID-19 is not a reason to deny admission.” Months later, nearly70 percent of coronavirus fatalities in the state have occurred in nursing homes.
Not being content with causing such a disaster, the state health department has issued guidance on how healthcare facilities should ration the limited supply of the new drug Remdesivir in the event that there are not enough doses to go around, but notes that the guidelines should apply to any scarce form of treatment. While certainly an unpleasant subject to address, it is true that in the face of scarcity the limited supply of Remdesivir or any other treatment will need to be rationed and that some kind of method of choosing will be needed. Scarcity is simply a fact of life that must be dealt with. However, because the distribution of Remdisivir has been taken over by the federal government, which distributes it to state governments, which in turn distribute it to healthcare providers, the process has unavoidably become political.
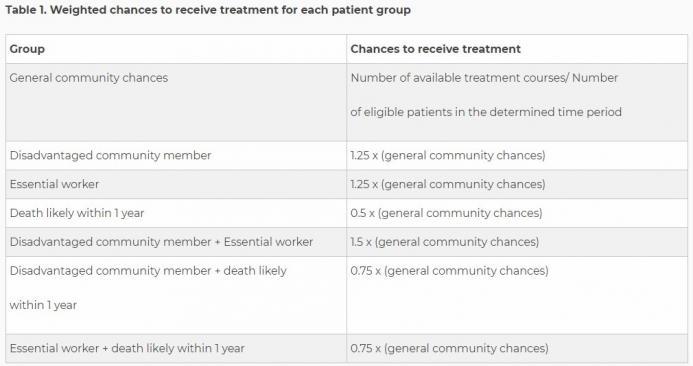
Putting all the jargon aside, the guideline is very clear about several points. First, it is not considered acceptable to distribute care via a random lottery, or on a first-come-first-served basis. Rather, healthcare providers must take into consideration “community-benefit” when rationing care and the department recommends the use of a weighted lottery system.
As you can see, the example lottery that the health department provides uses three different criteria to determine how a patient’s lottery chance is weighted: membership in a disadvantaged community, being an essential worker, and likelihood of death in the next year.
While the state’s determination of who is and who is not an essential worker is arbitrary and has been full of problems, one can at least see the logic behind such a consideration, as well as for those patients who are not likely to live much longer, although one must question where the state gets the authority to dictate such things to hospitals.
What raises the most concern is the idea that members of “disadvantaged communities” should be given a better chance at receiving treatment than others.
According to the guidance, because “low-income communities and certain racial/ethnic minorities” are being disproportionately burdened by the coronavirus, the end goal of public health is served by benefitting some groups over others.
According to the guidance, “the rationale is that a core goal of public health is to redress inequities that make health and safety less accessible to disadvantaged groups.”
One might have thought that the main goal of public health was to save as many lives as possible. But instead, it seems that the state department of health considers the emergency room to be the perfect place to start “mitigating the structural inequities that cause certain communities to bear the greatest burden during the pandemic.”
This formulation makes it unclear what the guidance means when it states that the first goal of the ethical framework is “to safeguard the public’s health by allocating scarce treatments to maximize community benefit.” Does community benefit mean saving as many lives as possible? Or is it some kind of grievance studies conception of equality where arriving at a more “equally distributed” survival rate based on race and socioeconomic status is the goal?
One can certainly argue that certain populations do not have very good access to healthcare resources, but it seems outrageous to think that the time to attempt to remedy such inequality is when triaging patients.
Similarly concerning is the way the guidance recommends that the treating physicians be removed from the rationing process and that it be left in the hands of hospital bureaucrats instead, effectively tying doctors’ hands to treat their patients. Is this the kind of state-run healthcare that we have to look forward to in the future? Doctors as helpless as their patients as bureaucrats “assess” a patient’s social suitability to be worthy of treatment?
The guidance goes on to recommend some procedures for how membership in a “disadvantaged community” should be determined. After noting that both members of low-income communities and racial minorities have been adversely affected by the virus and therefore deserve an increased chance of receiving treatment, the racial component drops entirely from consideration in recommendations, no doubt because such discrimination would be highly illegal and result in a torrent of lawsuits against the state and any hospital foolish enough to try it. The guideline is explicit that “no one is excluded from access based on age, disability, religion, race, ethnicity, national origin, immigration status, gender, sexual orientation, or gender identity and to ensure that no one is denied access based on stereotypes, perceived quality of life, or judgments about a person’s worth.” However, one can’t help but think that if racial discrimination were not illegal the logic of this guidance would dictate that it be undertaken in the name of “equality.”
What that list is lacking is a prohibition on discrimination based on socioeconomic status, which is the method the guidance suggests should be used for the purposes of weighing the lottery. Specifically, it recommends the use of the Area Deprivation Index, which is based on data from the 2015 American Community Survey. Hospitals would use the index’s Neighborhood Atlas to enter a patient’s address and determine if they are a disadvantaged community member.
One can’t help but feel that such a system is arbitrary to the extreme. When I entered my address into the Neighborhood Atlas I discovered that no one in my neighborhood would receive any weighted advantage if Remdisivir were needed. However, when I Google mapped the distance between my home and the nearest sector considered to be disadvantaged, I discovered that it was a mere two-minute drive away. Can anything based on something so arbitrary as five-year-old aggregated census block data be considered a useful tool for the fair rationing of treatment?
This entire scheme is just a taste of the ways medical care would be infected with politics if it were to be run by the government. In a system of socialized medicine would we see similar redistributionist schemes of rationing introduced? No doubt, many people of all political persuasions would view it as a fertile field for attempts at social engineering. Similarly, it is not hard to see politicians scheming to ensure that favored constituents and voting blocs have access to care at the expense of their opponent’s supporters, or that whole classes of people are purposefully and consciously disadvantaged based on whoever holds the keys to power at the moment.
The middle of a pandemic is no time for social engineering, but it is also not a time for state involvement in healthcare to begin with. That involvement has led to thousands of nursing home patients dying and has now led to a blatant redistributionist drug-rationing scheme. Further involvement is only going to make matters worse and continue to poison a crucial aspect of our lives with politics even more than it already is.
via ZeroHedge News https://ift.tt/31FIx5O Tyler Durden
Mississippi School Reopens Only To Send 100 Students Home When Teacher Appears Sick Tyler Durden
Tue, 08/11/2020 – 21:05
School districts across the nation are on edge now that we’re entering mid-August into September, when K-12 schools typically open. And during more normal times Fall sports like football are already in full swing in terms of practices, which in some places, for example in most parts of Texas, appears to be resuming as normal.
Many districts especially in the South are offering an ‘online option’ especially for middle through high school students while simultaneously opening their doors, albeit with strict safety measures in place, such as temperature checks and the wearing of masks.
But one Mississippi public school opened its doors as scheduled in early August, only to now be living the nightmare that most fear: “Roughly 100 students were sent home from a southern Mississippi high school on Tuesday after coming into contact with a teacher who was exhibiting mild COVID-19 symptoms,”The Hill reports.
Gulfport High School in Gulfport, Mississippi, via WLOX News.
Amid raging school board debates and varying opinions among administrators over re-opening, many who say schools should stay closed altogether this fall argue that the moment a cluster of COVID-19 confirmations emerges in any given school they are going to shut their doors anyway.
In this latest case in Gulfport, Mississippi it’s not even as yet clear whether the teacher actually has coronavirus. But while a test is pending students were sent home anyway “out of an abundance of caution to keep everyone safe,” the district said in a statement.
Any students and faculty that had contact with the teacher will enter a 14-day quarantine – again estimated at about 100 – not returning to campus, pending the teacher’s test results return, The Hill continues. In the case of a negative test, the school said classes will resume as normal. The school says social distancing measures have been in place.
The whole episode presents a serious dilemma which high schools and hesitant colleges are sure to experience: assuming a school reopens, how much panic will ensue the moment students and teachers naturally catch common colds or other viruses?
Stock image: Infection Control Tech
Outbreaks of various types of illnesses, or coughs, or also bacterial illnesses like Strep throat tend to be all-too-common on school campuses particularly in the fall and winter months.
It begs the question: will schools go on lockdown every time someone catches a common cold?
Add to this scenario the concern that many doctors and health officials have expressed, namely there’s a greater likelihood that after multiple months of much of the nation staying at home and social distancing, people’s immune systems tend to be much weaker, and thus could experience a ‘shock’ of sorts (in the form of illness) the moment individuals are back among crowds.
via ZeroHedge News https://ift.tt/3fOJEVV Tyler Durden
The bill, introduced by Sen. Thom Tillis (R-NC) and supported by the International Council of Shopping Centers, would allow for the facilitation of commercial tenant rent deferrals and providing additional flexibility for small business tenants that file Chapter 11 bankruptcy.
“The legislation will help businesses struggling with bankruptcy to weather the storm,” ICSC president and CEO Tom McGee said. “The bill provides significant relief to small business debtors and landlords. It also reinforces what many landlords have done since spring, as well as encourage deferred deals going forward.”
Under current law, rent deferral agreements waiving some or all of the current rent to be repaid in the future can be undone if the commercial tenant later files for bankruptcy. This risk discourages such agreements from happening. Specifically, Bankruptcy Code Section 547 deems the installment payments as “preferences” and commercial landlords can be forced by the court to forfeit such payments.
The Tillis bill would prevent this from happening, providing “certainty” to business landlords, as well as tenants, according to ICSC.
Additionally, the Tillis bill would allow an extra 90 days for commercial tenants in bankruptcy to decide whether to continue with current leases. And for certain small businesses, the bill would give tenants the ability to spread the payment of some post-bankruptcy rent over a longer period. The extra time would provide liquidity to small businesses, preserving jobs and businesses, noted ICSC.
As we reported previously, a parallel attempt to bail out the ultra-rich investors who are holding impaired commercial mortgage-backed securities was introduced by Reps Van Taylor (R., Texas) Rep. Al Lawson (D., Fla.). According to the initial proposal, and as usual, taxpayers would end up being on the hook via the various Fed-Treasury JVs that will fund these programs, as any new money injected to rescue CMBS debt will by default be junior to existing insolvent debt as “many of these borrowers have provisions in their initial loan documents that forbid them from taking on more debt without additional approval from their servicers. The proposed facility would instead structure the cash infusions as preferred equity, which isn’t subject to the debt restrictions.”
via ZeroHedge News https://ift.tt/3kAGTeu Tyler Durden
Russian President Vladimir Putin announced today that Russia has won the global race to be the first country to produce and officially register an effective vaccine against the COVID-19 coronavirus. Putin also said that one of his daughters was a vaccine test subject who experienced a couple of days of fever after being inoculated but is now feeling well.
The absence of publicly available data and the speed with which the vaccine has been approved have alarmed researchers and public health authorities around the world. “This is a reckless and foolish decision. Mass vaccination with an improperly tested vaccine is unethical,” declares University College London geneticist Francois Balloux in Nature. “Any problem with the Russian vaccination campaign would be disastrous both through its negative effects on health, but also because it would further set back the acceptance of vaccines in the population.”
“If they get it wrong it could undermine the entire global enterprise,” agrees Baylor College of Medicine vaccine scientist Peter Hotez also in Nature. “Not sure what Russia is up to, but I certainly would not take a vaccine that hasn’t been tested in Phase III,” said Florian Krammer, an immunologist at Icahn School of Medicine at Mount Sinai in New York City, in a tweet. “Nobody knows if it’s safe or if it works. They are putting [health-care workers] and their population at risk.”
The vaccine has been dubbed “Sputnik V,” as an homage to another global technological victory by Russia’s Soviet predecessor state, the launching of the first orbital satellite Sputnik in 1957. Developed by the state-run Gamaleya Research Institute of Epidemiology and Microbiology in Moscow, the viral vector vaccine uses a common cold virus that is engineered to carry selected coronavirus genes as the way to provoke an appropriate immune response. So far Russian researchers have not published anyscientific data regarding the safety and efficacy of the vaccine.
Russian officials have reportedly suggested that mass inoculation focusing first on health care workers and teachers would start as early as October. Russian media also announced that the government had received requests from 20 different countries for the production of 1 billion doses of the vaccine.
U.S. biotech and pharmaceutical companies are rushing at warp speed to develop and deploy safe and effective COVID-19 vaccines. Some commentators have worried that President Donald Trump might try to pressure the Food and Drug Administration into approving a coronavirus vaccine before it’s ready as an “October surprise” to boost his chances in a tight election. “This just cannot be allowed to happen,” declared National Institutes of Health head Francis Collins on CNN today. Be that as it may, Vanderbilt University vaccine expert William Schaffner observed that Trump “has thrown the usual manual of how to function in a pandemic out the window” and Putin seems to be writing a new one.
from Latest – Reason.com https://ift.tt/31FTyUR
via IFTTT
Russian President Vladimir Putin announced today that Russia has won the global race to be the first country to produce and officially register an effective vaccine against the COVID-19 coronavirus. Putin also said that one of his daughters was a vaccine test subject who experienced a couple of days of fever after being inoculated but is now feeling well.
The absence of publicly available data and the speed with which the vaccine has been approved have alarmed researchers and public health authorities around the world. “This is a reckless and foolish decision. Mass vaccination with an improperly tested vaccine is unethical,” declares University College London geneticist Francois Balloux in Nature. “Any problem with the Russian vaccination campaign would be disastrous both through its negative effects on health, but also because it would further set back the acceptance of vaccines in the population.”
“If they get it wrong it could undermine the entire global enterprise,” agrees Baylor College of Medicine vaccine scientist Peter Hotez also in Nature. “Not sure what Russia is up to, but I certainly would not take a vaccine that hasn’t been tested in Phase III,” said Florian Krammer, an immunologist at Icahn School of Medicine at Mount Sinai in New York City, in a tweet. “Nobody knows if it’s safe or if it works. They are putting [health-care workers] and their population at risk.”
The vaccine has been dubbed “Sputnik V,” as an homage to another global technological victory by Russia’s Soviet predecessor state, the launching of the first orbital satellite Sputnik in 1957. Developed by the state-run Gamaleya Research Institute of Epidemiology and Microbiology in Moscow, the viral vector vaccine uses a common cold virus that is engineered to carry selected coronavirus genes as the way to provoke an appropriate immune response. So far Russian researchers have not published anyscientific data regarding the safety and efficacy of the vaccine.
Russian officials have reportedly suggested that mass inoculation focusing first on health care workers and teachers would start as early as October. Russian media also announced that the government had received requests from 20 different countries for the production of 1 billion doses of the vaccine.
U.S. biotech and pharmaceutical companies are rushing at warp speed to develop and deploy safe and effective COVID-19 vaccines. Some commentators have worried that President Donald Trump might try to pressure the Food and Drug Administration into approving a coronavirus vaccine before it’s ready as an “October surprise” to boost his chances in a tight election. “This just cannot be allowed to happen,” declared National Institutes of Health head Francis Collins on CNN today. Be that as it may, Vanderbilt University vaccine expert William Schaffner observed that Trump “has thrown the usual manual of how to function in a pandemic out the window” and Putin seems to be writing a new one.
from Latest – Reason.com https://ift.tt/31FTyUR
via IFTTT
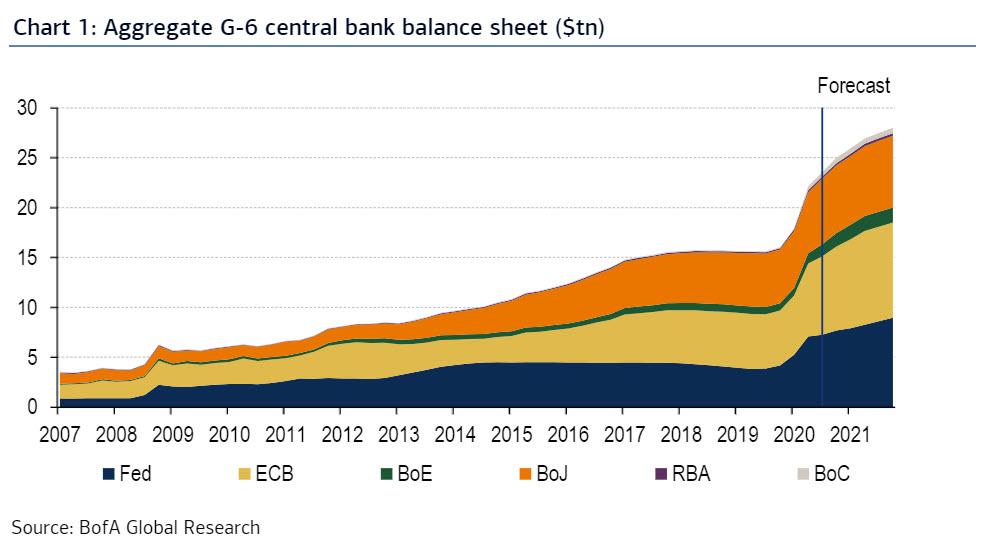
Central Bank Balance Sheets To Hit $28 Trillion Next Year Tyler Durden
Tue, 08/11/2020 – 20:25
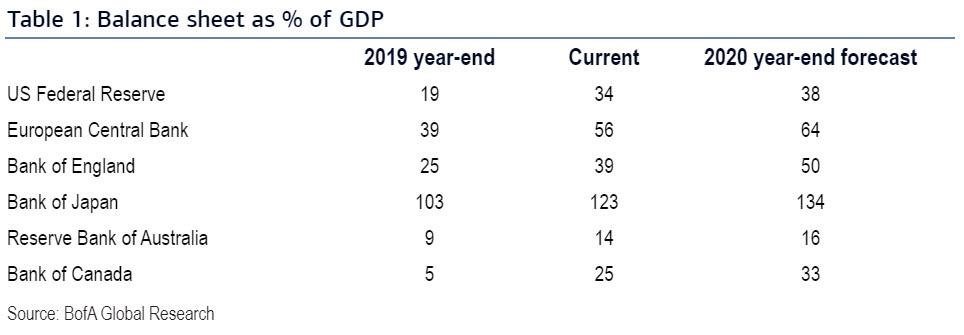
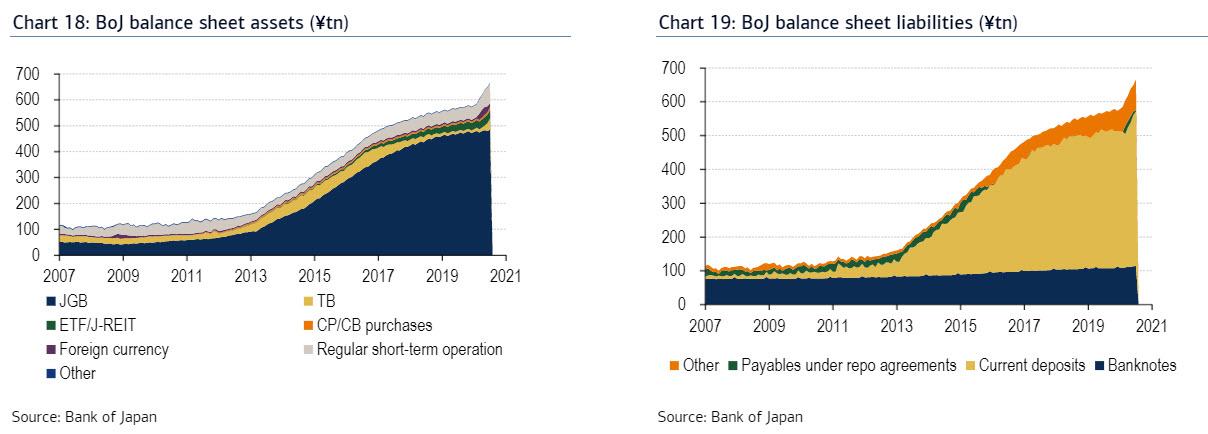
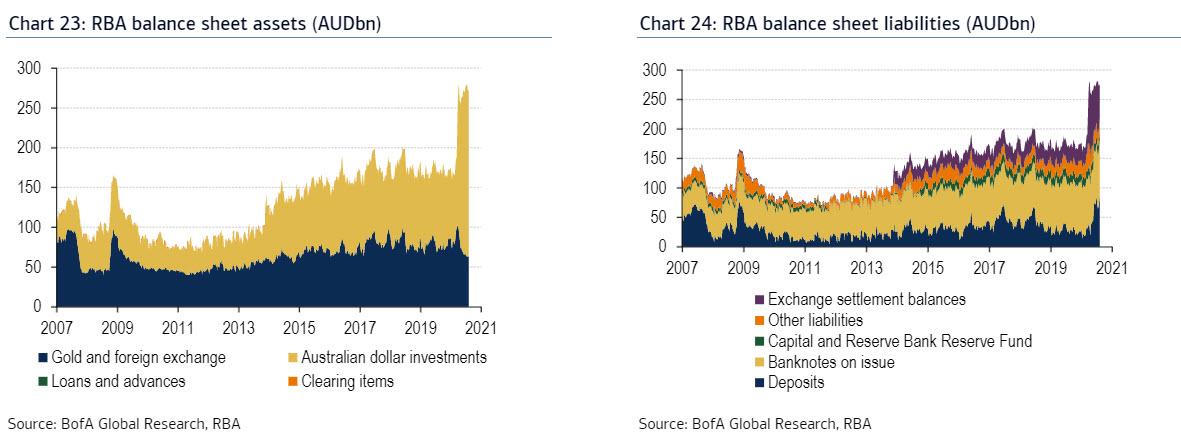
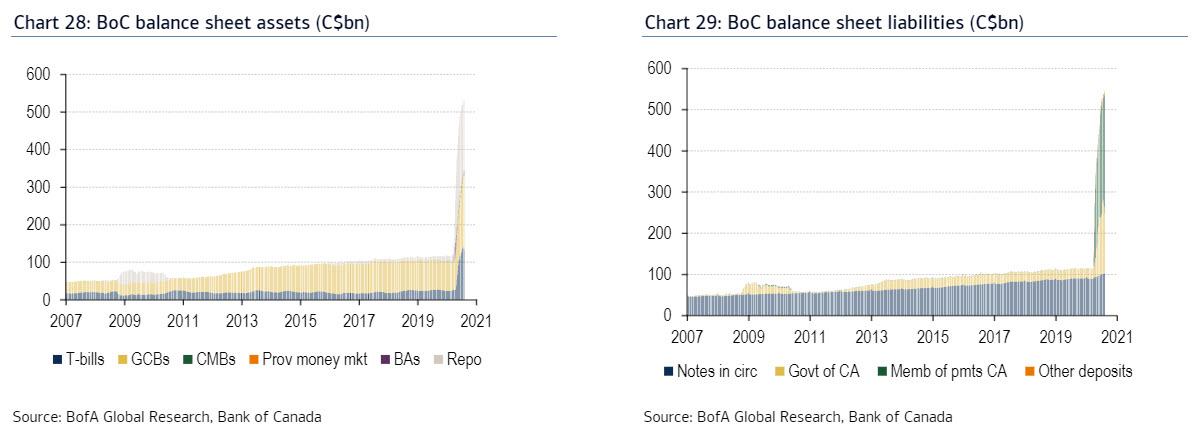
As noted earlier, silver is crashing as much as 15% today, a plunge which if it had spread to stocks would prompt a panic at the Fed and an injection of at least several trillion. The fact that precious metals do not need a rescue from the Fed – and in fact anything the Fed does do will only send them higher – is probably worth its own take, but for now we will simply look at how we got here, where we are going and update details on the balance sheets of the Federal Reserve, European Central Bank (ECB), Bank of England (BoE), Bank of Japan (BoJ), Reserve Bank of Australia (RBA), and Bank of Canada (BoC) balance sheets, as well as on the programs implemented by each central bank.
As BofA shows, central bank balance sheet have never been bigger with the Fed now “holding” 34% of US GDP, and expected to see this number rise to 38%. For the other central banks the number is 25% for Canada and 123% for Japan.
Putting an actual number to the liquidity firehose, central banks have injected $24 trillion, or about a quarter of global GDP, into the market to keep it from crashing and expectations are that this number will increase to $28 trillion by the end of next year (this excludes the tens of trillions in assorted liquidity instruments in China). That would be a very optimistic expectation.
And since these days chart inflation means that one picture is worth a trillion words, we will focus on the visuals as they are self-explanatory.
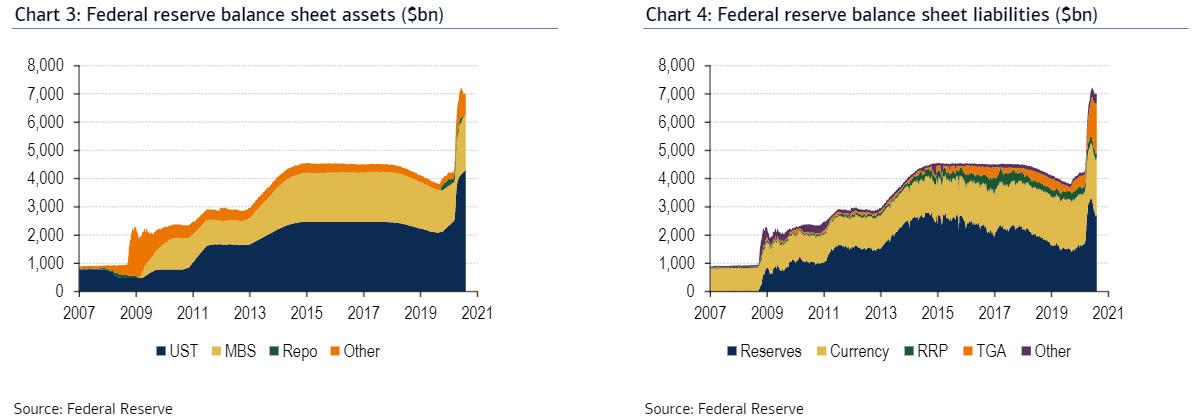
Fed:
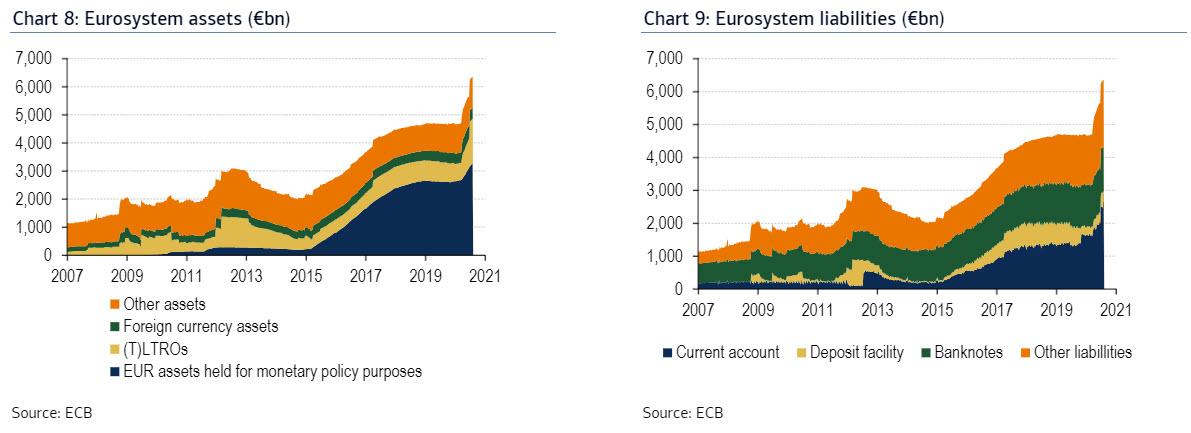
ECB:
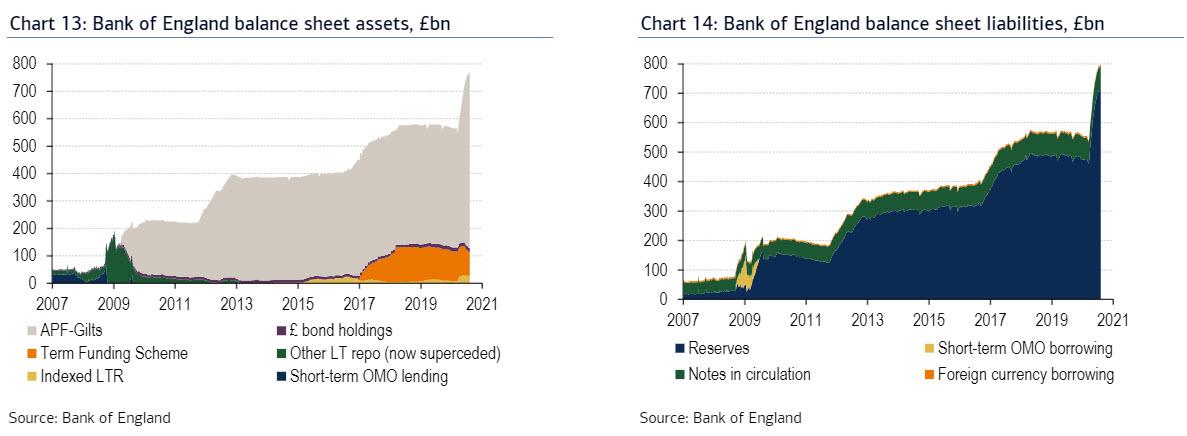
BOE:
BOJ:
RBA:
BoC:
via ZeroHedge News https://ift.tt/2XTRKq5 Tyler Durden
Of late, despite flashes of social media mania, there has been heartening focus in a number of countries from policy makers on evidence based COVID responses, localized interventions where needed, encouraging prudent social distancing and hygiene measures. This deserves to be supported.
An Orgy of Incoherence
Each day, in “COVID panic land” statements are issued that are never seemingly challenged, or even questioned, or even unpacked, or even “quizzed” for minimal coherence.
First, just a canopy bit of perspective, quoting Lord Sumption, former High Court Judge in the UK, who has become a lightning rod for speaking out about the mass invalidation of civil liberties over hyped hysteria.
“COVID-19 is a serious disease, but historically it is at the bottom end of the scale. For anyone under 50 the risk of death is tiny, less than for seasonal flu. In the great majority of cases the symptoms are mild or non-existent. Our ancestors lived with far worse epidemic diseases without rushing to put their heads in a bag. In other parts of the world they still do (world-wide, tuberculosis kills many more than COVID-19).”
While there is some outrage evident in Lord Sumption’s assessment, the above statements are all factually true, and can be objectively corroborated. Relative to our ancestral experience with viruses, I will spell that out further below as well, so as to pacify the “here and now” doomsayers.
Samples of Mindlessness
“What if COVID never goes away?”
Since it kills virtually no one in statistical terms below 60, and above 60 without comorbidities recovery rates are still highly encouraging, and since the impact on net mortality is not anywhere close to seismic on the actual numbers, the answer is, “We live with it.” Or “We end all life as we know it due to what is tantamount to a bad influenza period.”
It’s a virus, so likely may not disappear. We will develop greater immunity, our hygiene habits will improve, we might get a vaccine, but we need a “vaccine” against panic and the myopia of “risk-free” living, which we have not imposed on ourselves in reaction to anything else in history: from terrorism to earthquakes to tuberculosis to race car driving (so from the man-made catastrophes to natural disasters, to global diseases to human hobbies).
So, the question emerges, other than the now clearly discredited “optics” of warning us of millions of deaths, inflamed by modelers who have perfected the art of imperfection in their predictions (and our saying that is as “factual” as it gets), and other than reality being “gas-lighted” by deranged and virtually unremitting media reports urging panic and paralysis upon us, what triggers this bizarre new threshold of absurd self-preservation, even when the opportunity cost is the virtual end of social and economic life as we know it? We “sneezed” civilization away?
“What if there’s a second wave?”
It will, if following the patterns of virtually all viruses, be even less dangerous, immunity will be greater, we may be sane enough to protect nursing homes, and we will find the rebuilding of society a better place to focus our attention.
And why on God’s earth are we so infatuated with caseloads? A mild upward tick in Catalonia, and the UK in sheer panic imposes quarantine on anyone returning from Spain? Overall net mortality is no worse than the UK (zero in the last two days, August 1st and 2nd), and we are just postponing the inevitable, unless the UK is going to not only leave Europe but take leave of its senses at the same time, and operate as an “anti-COVID fortress” with dwindling economic and cultural and social prospects.
“But, by God, I’m NOT getting a fever or a dry cough, forget number of deaths annually by influenza, pneumonia, crossing the street, diabetes, heart attacks… all acceptable EXCEPT the dread… theme music please!… scourge of “COVID!”
Vietnam, which marshaled its sanity and responses so remarkably and reports to date no deaths from COVID, found three residents infected in DaNang, after months of no local cases reported apparently, and in a fit of over-reaction, shut DaNang down, and evacuated the (mostly local) tourists from there. Elephant guns and mosquitoes come to mind. (Several days later, updating on August 10th, there are now 11 deaths in Vietnam, averaging about 20 cases a day for the last few days; compared to anywhere else in the world, scant argument for panicked evacuation or shutdown).
Some large global multinationals have proclaimed no face-to-face meetings, even if crucially needed in local markets, until 2021! On what basis? Surely, this should be assessed locally? And if you are in a community which is recovering, now has 1,000 people gathering thresholds, or marriages of up to 500 or more taking place in Asia, and if you are a newly forming team that needs to engage, to rally, to align, to build the necessary relationships for greater virtual work to be possible, in fact, why would a HQ “declare” themselves a medical authority on gatherings per se, large or small, decoupled from the leadership discretion of leaders you have entrusted brands, livelihoods of your employees and hundreds of millions (or more) dollars in revenue to? And should not a “factual” threshold, rather than a calendar one be established?
We surely cannot manically shut down whole communities when infection rates and lethality rates show a serious but statistically modest viral challenge. But the economic meltdown, psychological impacts, social disruption, while not reducible to lab results, are every bit as palpable, arguably more devastating in the medium to longer term, and will not recover if societies and economies are being turned “on” and “off” by every “spasm” of control fetishism.
And the “Facts” Keep Rolling In
Just taking the “florid” Floridian over-reaction, a cursory look at July 25th shows 124 deaths reported, of which only one, only one I reiterate, took place that day! The rest were merrily backfilled from May 28th cumulatively! Should this not be taken as scandalously distorting? No, just another day in the “porn media” sweepstakes. As I write (August 2nd), hospital capacity in Florida is greater than it was on July 2nd, despite 300,000 tests administered since.
We also hear from numerous studies, including from Professor Francois Balloux in a pre-print, reconfirming evidence that eight out of 10 who never had COVID-19 seem to have an immune response triggered by T-cells based on prior exposure to other illnesses, including the common cold. That would argue for an affinity between this coronavirus and other more common strains, rather than this being a world ravaging contagion unlike any seen before. One wonders if we never encountered a virus prior to 2020?
Hot on the heels of that, The Wall Street Journal reported: Flu wiped out in Southern Hemisphere virtually, from reports. As an example, Chile had recorded as of the time of the article going to print, 1,134 respiratory illnesses compared to 20,949 last year. Could it be that people diagnosed with flu or influenza are being “tagged” as COVID-19, particularly those who die, hence the cases of flu and influenza seem to be on a precipitous decline?
As the plummeting numbers of seasonal respiratory viral infections from Argentina to South Africa to New Zealand continue to confound, the myopic are congratulating draconian COVID containment measures for this positive byproduct, ignoring the far more likely rationale that these are still there, “baked” into the COVID numbers. After all, other than via notoriously fallible tests, based on the symptoms, how could you know?
Once More a Plea for Perspective
Despite only 2% of DC’s hospital capacity being utilized, school has been cancelled for the fall due to the demands by the teacher’s union. With overwhelming global evidence of school openings being unconnected with any spikes thereafter, children not being at risk by and large (statistically being far more likely to be killed riding over to school, and over nine times as statistically likely to drown — source CDC — than from deaths “ascribed” to COVID), we have to more than wonder. Specifically, in the US,138 COVID “ascribed” deaths in that age group versus 995 from drowning in an average year, 4,000 in auto accidents for school age kids and teens over a similar period.
The Lancet has now also weighed in that Lockdowns don’t work, in a country by country analysis. But we already knew that! Just compare Japan to Belgium! Compare Taiwan to the UK. And we’ll get to Sweden, as fatality numbers plummet, and it was the only western country to have grown economically last quarter (Taiwan grew first quarter 2020, too). But for some reason we should insist rather that our “poster children” for COVID rectitude should be the shattered economies with no viral “breakthrough” to show for it? Virtually all of Europe has said, no hardcore lockdowns going forward, localized restrictions, prudent, evidence-based reactions, and following key elements of the Swedish model, would be the essential playbook.
As a percentage of the global population, even with all the likely “mis-stated” COVID fatalities, taking the numbers as gospel, we come in at .0052%. Swine Flu (2009–10) was .0029%, HIV .565%, Hong Kong flu of 1968 also much higher at .027%, Asian Flu of 1957/58 still higher at .070%, the Spanish flu of 1918 a ravaging 2.73%. The global economy persevered, the world progressed and moved on to fresh prosperity through all of these. Just yesterday we read the sheer collapse of GDP in the US has eliminated the last 5 years of growth in one fell swoop in a matter of months.
For those who relish historical comparisons, the true pandemic “terrors” were the Black Death of 1347–51 with 42.11% as a percentage of global population and the Plague of Justinian 541–542 with 28.51%. Doubtless the rudimentary understanding of medicine in those eras was a sharp contributing factor to the exponential growth of the respective contagions.
The Perpetuation of Fraudulent Panic-Mongering
Though mass congested protests are seemingly of no “superspreader” concern through some unexplained medical voodoo (pandering for political advantage being one of the “vaccines” against public health nostrums it seems), when “panic” seemed on the wane, mainstream media stopped tracking “deaths” (despite even those being periodically miscounted as per the CDC or back-filled), and decided that all “infections” past or present would now be anointed “new cases.” And voila, the floodgates are open once more via some linguistic legerdemain.
Not sick? No problem! No symptoms? Easy. Symptoms which could be mild and seasonal? You dare not make light! Not dying? Give it time… stop society!
Then came the mask mandates. We all know about them, so let me simply make the point that they are far from settled science, and they are downright dangerous when exercising, as the deaths of several Chinese students while running a race during PE with these contraptions heart-breakingly revealed.
The Norwegian health authorities, not noted for their reckless or libertine ways (and with some of the best COVID stats in Europe), doubled down recently on their recommendation for those without symptoms not to wear face masks, arguing the number of infections in Norway made them moot.
Taking the most optimistic efficacy number, medical masks prevent roughly 40% of infections. Keep in mind that most of us outside the medical profession are not wearing medical masks. 200,000 would have to wear them to prevent one new infection per week in Norway. As the agency wrote,
“The number of people who experience undesirable effects (difficulty breathing, communicating when that is critical, or dropping other hygienic prudence being given a false sense of security) is likely to be much larger than the number of infections prevented.”
They concede that in congested community settings, public transport etc., there “might” be some benefit, but again largely with medical masks. They note even then, “However, study results vary greatly.” This meshes with the recent conclusion from the Dutch government indicating they will not require universal mask wearing as effectiveness of overall “masking” has not been demonstrated to their empirical satisfaction. Oxford University points out that no government should be able to mandate this usurpation of civil liberties for something that is not “settled science” by any stretch of the imagination, based on observational assertions. The suggestion is that “liberties” are not to be trifled with, or annulled absent overwhelming “evidence” not assertion.
The Great Lockdown Lacuna
There was a gaping policy hole that “lockdown” sought to furtively fill, the pseudo-scientific reflexive obeisance to untested modeling.
From the reliably inaccurate doomsday prognosticator Neil Ferguson had come the “second Spanish flu” prediction (which had led to 50 million deaths when the world’s population was a fraction of today’s, roughly 1.7 billion, one third of which became infected) re COVID, predicting 500,000 deaths in the UK alone, and if Sweden continued its flirtation with disaster, “at least” 80,000+ there. Since Sweden has less than 6,000 deaths with no lockdown and 75% of those were from nursing home cases which they tragically mismanaged, and as we have countries that have not locked down, which have not produced such torrents of mortality, perhaps we can leave the modelers alone at last?
Even by the end of February, the Diamond Princess Cruise Ship provided a perfect sample to extrapolate from. And this was evidence-based, not model-based. 3,711 passengers and crew, quarantined after a virus outbreak, with an average age of 58 were repeatedly tested. There were 705 cases (19% infection rate), 6 deaths (case fatality rate of 1%) by the end of March, eventually 14 in total, compared to the 116 that the Imperial model would have predicted.
Over half the cases were “asymptomatic” which, if you take it at face value, meant many more were infected or “had” been infected, and the tests were picking up residue of the virus (which we are told can be detected for up to two months after it is no longer “live”). Either way the mortality rate would then resemble “severe seasonal influenza” as a saner version of Anthony Fauci had himself written earlier in the New England Journal of Medicine.
Almost all the deaths on the Diamond Princess were in the over 70 age group. Later the USS Theodore Roosevelt produced one death and three hospitalized cases out of 1,156 infections (much younger and healthier profile, of course), no deaths out of 1,046 cases on the Charles de Gaulle either, and this pattern continued to repeat.
WHO itself had added to the panic due to a rookie computational error, asserting the population mortality risk to be 3.8%. They arrived at this by taking the then known Chinese deaths and dividing them by the number of confirmed cases, ignoring that likely only a small proportion of infected people had been tested, asymptomatic cases were likely not represented, and those who went in for testing were inevitably those with serious symptoms. This evident computational distortion contributed also to the policy errors relating to both hospital capacity and nursing home fatalities.
Deaths in care homes are now estimated to have accounted for half of all COVID related mortality. When it was suggested, looking at 96% of Italian mortalities, for example, coming from the elderly with comorbidities, that we isolate the vulnerable, and not shut down the planet, people said it was “unrealistic” and “had never been done.” As if closing down the world, putting the wider economy into enforced seizure with no possible available longer-term financial hedge by which to recover livelihoods and industries, was a sane alternative?
For perspective, 650,000 COVID deaths globally pale next to 33.4 million deaths to date roughly in 2020 overall, and for most of the population (under 65 with no pre-existing conditions), normal influenza, road accidents, suicides, and a host of other causes of death (TB, cancer, hypertension, diabetes) are statistically far more significant. But the newness of COVID and the frenzied, fevered, unrelenting media hype have stripped most people’s critical faculties of any proportionality on that front it seems.
Though Stockholm with 2.5 times the population density of New York State outperformed NY State on virtually any COVID metric you care to name overall, and at their respective peaks, and therefore still has a relatively open economy today, far more so that NY State, when facts made it evident the virus had all but disappeared from Sweden, there was from the media enablers and all the governments and who had clung feverishly to the “lockdown” mania, not a word, just deafening silence.
Researchers from the University of Toronto found that whether a country was locked down or not was “not associated” with the COVID-19 death rate. The noted journal Lancet cites,
“Government actions such as border closures, full lockdowns, and a high rate of COVID-19 testing were not associated with statistically significant reductions in the number of critical cases or overall mortality.”
They did plausibly keep, for an initial period, hospitals from being over-run, and that should certainly be evaluated in a focused way on that basis.
The Bad Science Round Up
Forcing people walking in parks to wear masks, when even the most fantastic assertions of aerosol transmissibility, which came from machines in lab settings, do not suggest in open air, a mere cough or exhalation magically can be infectiously propelled to unwitting passerby, is moronic.
Swedes and Danes and the Dutch have been enjoying social interaction in cafes and bars, but don’t let the Irish near those pubs (August 10th may see that finally relaxed). As one commentator mentioned, they doubtless have an obscure Irish custom we don’t know about and they need to be weaned off, that in riotous affection leads them to kiss each other’s noses and hack into each other’s throats whenever in pubs. Otherwise, what happens on “August 10th” that wasn’t true on “July 10th” seems quite inscrutable.
Melbourne has interrupted its last “Level 3” Lockdown to initiate a new six week “Level 4” Lockdown (replete with overnight curfew) due to the admitted concern of 600 or so cases of what they are calling “community transmission.” But the real precipitating panic during this “surge” was apparently the number of deaths in a 24 hour period. That number is “seven” during a 24 hour period (considered “recovery” numbers in much of the planet) and still the overall COVID ascribed death count for Australia is 208 from February across the entire country! Those seven, were 70, 80 and 90 years of age, with numerous pre-existing conditions. The fragility of the economy there does not suggest immunity to other shocks likely to flow from these overlapping, never ending lockdowns, particularly as it’s winter there, and viruses are known at times to naturally spike over that period.
And why don’t we finish yet another round-up of our fevered over-reactions with the precarious petulance of the “tests” by which these dire read-outs emerge at all?
Professor Carl Heneghan, Director of Oxford’s Centre for Evidence Based Medicine, provides a bracing corrective, indicating that at lower prevalence of the virus, “sensitivity” and “specificity” of the testing gets less precise.
You start first with the “sensitivity” of the test: the proportion of people who test positive out of those who actually have the virus. The second is “specificity” which is the proportion who test negative, out of those who should indeed have done so. The true specificity and sensitivity of the prevailing tests are not known, admitted to by the UK’s Office for National Statistics, owing to the newness of the virus, a tripwire shared globally.
Let us take the Professor’s operating theater of the UK and assume 1,000 people have the virus, say, .1% (current actual estimates are lower, hovering around 0.04%). Now, say, 10,000 random people go get tested. So, 10 people will have it at the 0.1% infection rate, and 9,990 will not. Estimates tell us 80% of those who have the virus test positive, says the Professor (easily corroborated), this is the “sensitivity” and the “specificity” for those who test negative may be as high as 99.9% with the best (rare) tests.
So, on this basis, eight people will be correctly identified, and two will receive a false negative.
Of the 9,990 that are actually negative, all but 10 will be correctly diagnosed as “negative.” But 10 will be told they have COVID-19 when they actually don’t. That gives us 18 positive tests; eight from those who have it, and 10 from those who don’t. So only 44% of the infections indicated are real. Hence, we have to say, alarmingly, the chance of accurately detecting the disease being less than 50% is fairly glaring.
This isn’t hypothetical, as current viral levels are lower than the above case study. The US Centers for Disease Control kits concede they can generate up to 30% false positives! With the top tests costing upwards of GBP 100 per test, developing countries necessarily opt for more affordable options, with tests where specificity could be as low as 95%.
Then in the 10,000 test scenario, there would be 500 false positives among the eight genuine positives, so the false positives would far outstrip the genuine results, providing an appearance of a “surge” in infections that seems mystifyingly disconnected from numbers of hospital admissions and deaths.
So, if at low prevalence, with false positives rising at the same time actual infections plummet, then even if COVID-19 completely disappeared (the aspired to promised land), then even with no actual positives, on the above example, ten people would be wrongly diagnosed as positive, and the official data would obstinately still show a 0.1% prevalence of COVID-19! Off the current testing regimes, we may be incessantly chasing a shadow, and we may endlessly perpetuate panic and social and economic meltdown over a veritable phantom as a result.
Therefore?
It’s time to restate terms of reference and redefine thresholds meriting panic. We must clarify actual mortality and not “caseloads” as the relevant metric and compare cost/benefit trade-offs rather than allowing ourselves to be economically devastated and medically cuckolded by episodic ephemera posing as data.
via ZeroHedge News https://ift.tt/3aiCxnG Tyler Durden








{kind=link}
{kind=link}